Huntington’s disease is a genetic condition that impacts the brain and, over time, affects a person’s ability to control the movement of the arms, legs, face and torso (called chorea). It can lead to changes in personality and mental health and, over time, dementia. It begins most often in adulthood. As the disease progresses, the symptoms continue to get worse, as a person loses the ability to walk and talk and eventually develops muscle rigidity (tightness) and severe dementia. Among genetic disorders, the Huntington’s disease inheritance pattern is not typical, but more about this shortly.
What is the Inheritance Pattern for the Huntington’s Disease Allele?
The gene responsible for Huntington’s disease (HD) is called HTT. It produces a protein called huntingtin. Although the exact function of the protein is not known, it is believed to play an important role in the nerve cells in the brain. These cells send electrical impulses through the brain and other parts of the body that allow you to make moves like raising your hand or wiggling your toes. Individuals with HD produce an abnormal HTT protein due to a mutation in the HTT gene that causes the nerve cells to malfunction and stop working. This causes parts of the brain to start to wither away (atrophy), leading to the disease.
Autosomal Dominance: Inheritance Pattern for Huntington’s Disease
Everyone has two copies of HTT, one from mom and one from dad. At the very beginning of the HTT gene, there is a repetitive part of the genetic code. Specifically, three genetic building blocks (called base pairs), Cytosine-Adenine-Guanine, are repeated over and over again in that order: CAG, CAG, CAG and so on. For this reason, HD is known as a triple or trinucleotide repeat disorder.
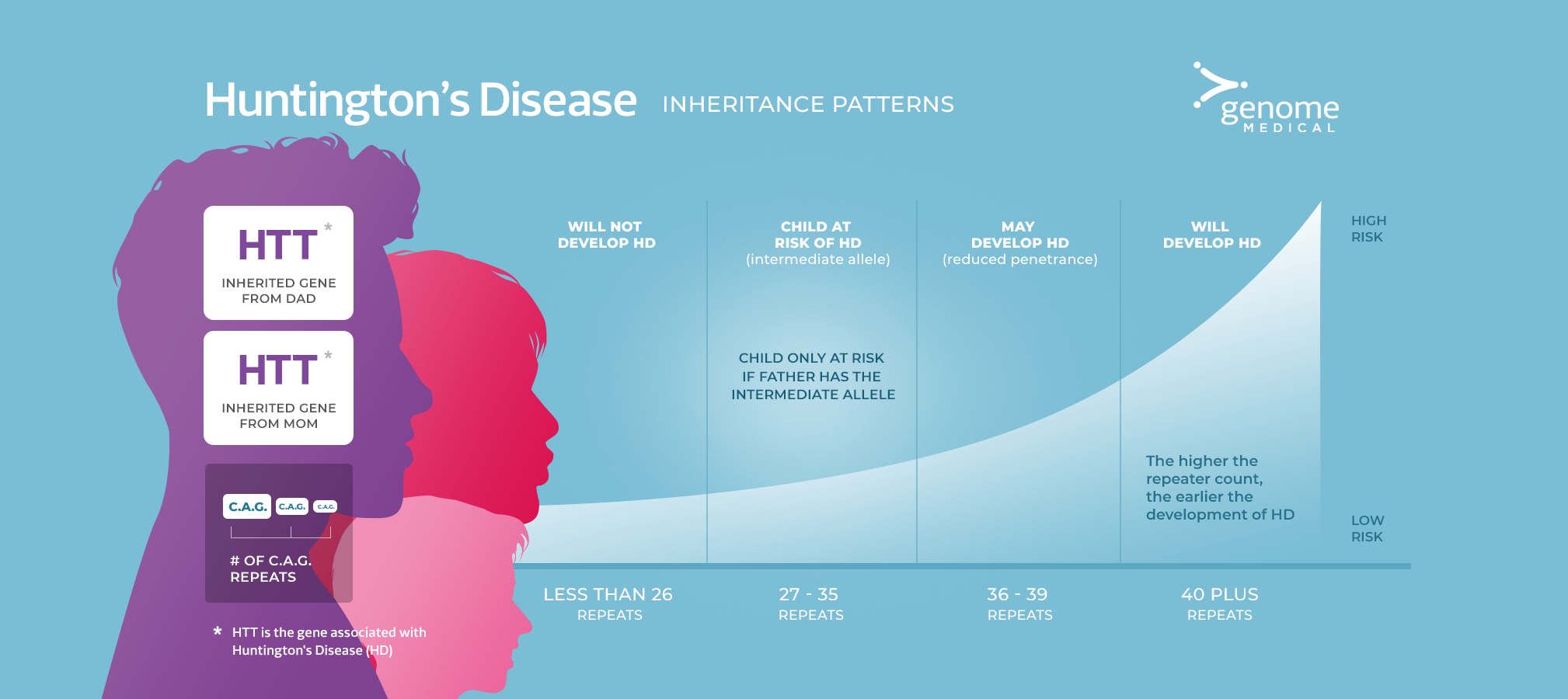
Number of CAG Repeats
People who are not at risk of developing HD have 26 or fewer CAG repeats in their HTT genes. Individuals who have between 27 and 35 CAG repeats are not at risk of developing HD but could have a child who is at risk of the disease. (This repeat range is called an “intermediate allele”, with the term allele being another word to describe a gene.) Individuals who have 36 to 39 CAG repeats may or may not develop HD (this is considered a “reduced penetrance” allele). If someone in this category does develop HD, it is generally at a later age. Lastly, individuals with 40 or more CAG repeats will definitely develop HD, and the more CAG repeats someone has, the earlier the disease will appear. For instance, when the CAG repeat size expands to 60, HD can start in the teen years.
Role of Sex in the Inheritance Pattern
HD is an autosomal dominant condition; this means that anyone who has a CAG repeat size of 40 or more has a 50% chance of passing the risk of developing HD on to their children. However, what makes HD unique among autosomal dominant disorders is that the size of the CAG repeats can get bigger when passed from parent to child — but only when passed from fathers to children. For example, if a man has a CAG repeat size in the intermediate range (say 35), his children could have a CAG repeat size of 40 and develop HD, even though the man will not develop the disease. Therefore, in families where the CAG repeat expansion is being passed through males, the age of onset can become earlier and earlier because the CAG repeat can expand. This pattern — when the age of onset gets younger and younger through the generations — is called anticipation.
Diagnosing Huntington’s Disease
Genetic testing of the HTT gene can determine a person’s CAG repeat sizes and assess the chance of developing HD. Deciding whether to undergo genetic testing for this disease is never an easy decision. There is no cure or prevention for HD; treatment typically involves managing symptoms as they develop and progress. While Huntington’s disease can be a devastating diagnosis to individuals and families alike, for the first time in a while, there are some new drugs in clinical trials that may provide some promise in treating HD.
Some people choose to be tested for HD because they want to use the information for family planning purposes. There are now genetic technologies available that allow a couple who know there is a risk of HD to have a child without the condition. For example, in preimplantation genetic testing, a couple undergoes in vitro fertilization; when the embryos develop to a specific stage, a single cell can be removed and tested for HD. Embryos that do not have the CAG repeat expansion can then be implanted, virtually guaranteeing the birth of a child not at risk of HD.
In other situations, people may choose to be tested for financial and medical planning purposes. Some individuals may want to ensure that they have all of the necessary insurance, medical power of attorney and other estate planning in place so that if and when HD is diagnosed, the family has less of a financial burden and knows how to manage the individual‘s care.
Given the potential risk of significant psychological effects of testing positive for HD, it is extremely important that individuals meet with a genetics professional, a psychologist and other health care professionals before moving forward with predictive HD genetic testing.
